Just the Facts: Recognizing the Importance of Reporting Accurate Information in a Wilderness Emergency
March 10, 2025
In the movie Die Hard 2, hero John McLane, played by Bruce Willis, receives a fax at a car rental kiosk at Dulles International Airport in Washington, D.C. informing him of the identity of a suspect. The agent behind the desk, who’s been flirting with McLane through the entire scene, says, “Hey, I close in about an hour. Maybe we can go get a drink?” McLane smiles coyly, points to the wedding ring on his finger, and replies, “Just the fax, ma’am. Just the fax.”

McLane’s line is a reference to the old TV show Dragnet, where the main character, Sgt. Joe Friday, would remind rambling or opiniated witnesses to stick to the facts by saying, “Just the facts, ma’am [or sir]. Just the facts.” That straight-forward statement can serve as a reminder for wilderness medicine providers when we’re responding to accidents or emergencies in remote settings.
In wilderness emergency medicine, collecting and reporting the facts can determine the difference between a positive and a negative outcome, or even between life and death.
Recognizing the Challenges of Reporting Accurate Information in Wilderness Medicine
In wilderness settings, the potential for communicating inaccurate information increases due to several factors, including distance, time lags, layers of patient care providers, and unreliable communication channels, including the absence of cell phone connectivity. First responders frequently face the daunting task of gathering information from people in stressful situations under challenging and changing conditions. In our wilderness medicine course, we teach about the importance of accurate information.
In addition, location information can be difficult to obtain and communicate. Even in an urban setting, first responders can have trouble distinguishing between similarly named roads, such as Bear Hollow Lane and Bear Hollow Road, or roads that have multiple names. In the wilderness, determining and communicating a specific location becomes even more challenging when certain ridges, pitches of a rock climb, or similarly named streams come into play.
Providing accurate and comprehensive information is important for several reasons, including the following:
- To avoid medication errors, such as giving someone a medication they’re allergic to
- To help next-level providers prepare for the highest priority interventions
- To help next-level providers identify additional resources that may be needed
Sizing Up the Scene
In wilderness medicine communications, being concise, accurate, and factual — and keeping it brief — is important. A comprehensive and accurate evaluation begins with sizing up the scene, which involves gathering the following information:
- The number of deceased and injured parties
- The nature and severity of the injuries and the urgency of treatment
- Availability of resources (medical equipment and supplies; food, water, and other essentials; and human resources)
- The location (in the context of access to additional resources and/or evacuation)
- The nature of the terrain
- Weather conditions
Evaluating Ill or Injured Parties: History of Present Illness
An essential component of sizing up the scene involves evaluating the condition of the people at the scene. Conducting a history of present illness (HPI) ensures that all pertinent information about each patient is gathered:
- Chief complaint: The primary reason the person needs care, such as injury, illness, or symptoms like pain, dizziness, or difficulty breathing.
- Context and onset: How and when the injury or illness began. Consider the environment, activities involved (for example, hiking, climbing, or swimming), and any potential risk factors (for example, extreme weather or lack of resources).
- Mechanism of injury or exposure: The cause of the injury or illness, such as a fall, an animal bite, environmental exposure (heatstroke, hypothermia), or food poisoning.
- Symptoms and progression: The nature, duration, and severity of symptoms (for example, pain level, swelling, shortness of breath). Consider whether the condition has worsened or stabilized over time.
- Medical history: Relevant past medical history, such as allergies, chronic health conditions, or previous injuries that may influence current health status, especially when evacuation may be necessary.
- Risk factors: Any conditions that make the patient’s condition worse, such as high altitude, dehydration, infection risks, or exposure to extreme weather conditions.
- Assessment of immediate needs: Anything the patient needs immediately to preserve life and limb; for example, CPR, immobilization, or tourniquet, and how these interventions can be managed with available resources.
To create an accurate and comprehensive history of illness, question the individual you’re evaluating. One method of obtaining detailed information from a conscious patient is to use the OPQRST mnemonic to evaluate the nature and severity of pain:
- Onset: Ask questions such as “What were you doing when the pain started?” and “Did you feel the pain suddenly or did it develop gradually over time?”
- Provokes or palliates: Ask, “What makes the pain better or worse?” Anything that makes the pain worse provokes it. Anything that makes it better is palliative, meaning it relieves the pain.
- Quality: Ask, “How would you describe your pain?” You could ask whether the pain is dull and achy or sharp, but a more open-ended question is likely to elicit an answer that gives you more insight into the nature of the pain.
- Radiates: Say, “Point to where you hurt the most.” and ask, “Where does the pain go from there?” When pain radiates (spreads from one part of the body to another), it can indicate the source of the pain; for example, pain in the lower back that radiates down the leg is likely to indicate a spinal injury that’s stressing a nerve near the spine.
- Severity: Ask the patient to rank the severity of their pain on a scale of 1 to 10. Remember that pain is subjective. The severity of pain for the same injury can vary widely from patient to patient.
- Time: Ask, “When did the pain start?” or “How long ago did the pain start?”
Recording Details with SOAP Notes
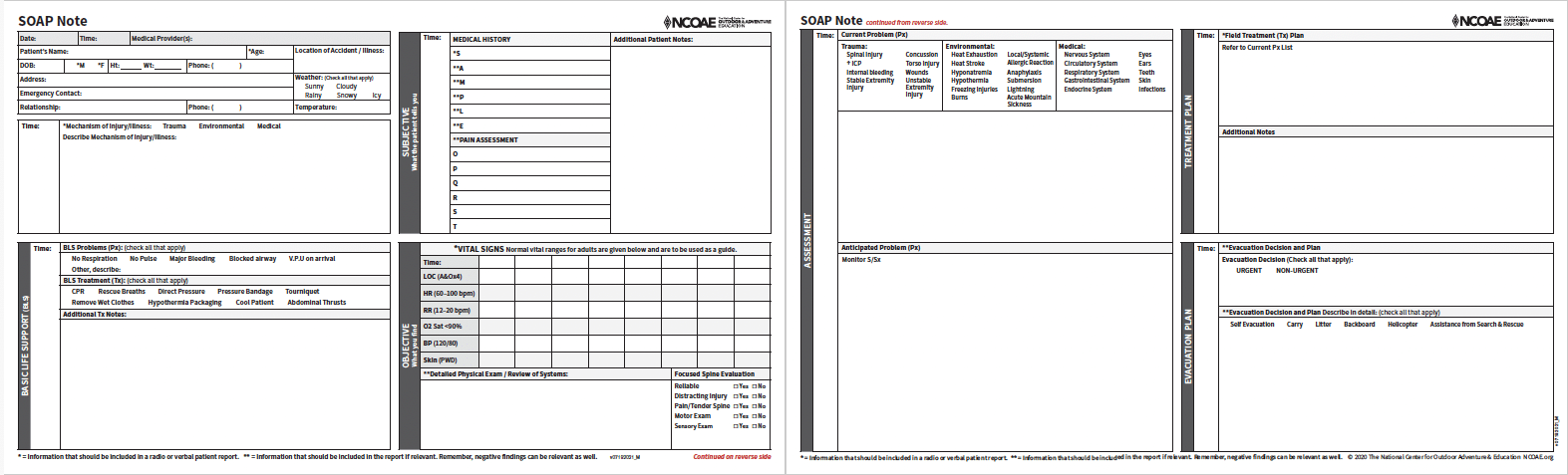
One of the best approaches to recording and reporting facts about an illness or injury in a remote wilderness setting is to use SOAP notes, as shown in the image below.
Complete a life-saving primary assessment and provide any urgent care necessary, such as CPR, prior to starting your SOAP notes.
SOAP is an acronym that stands for the following:
- Subjective: What the patient tells you about their medical history, pain level, and other relevant health/medical details.
- Objective: Vital signs, including heart rhythm, respiration rate, oxygen saturation level, and blood pressure.
- Assessment: Diagnostic details, such as whether the patient is suffering from a spinal injury, heat stroke, anaphylaxis, hypothermia, respiratory illness, or some other condition, along with concerns about any anticipated problems.
- Plan: The planning portion of SOAP notes covers treatment and evacuation. Note any treatments provided, such as cleaning and bandaging a wound, providing medication, and rehydrating a patient. For evacuation, note the urgency of evacuation and the recommended means, such as self-evacuation, carrying the patient, calling in a helicopter, or getting assistance from a search and rescue team.
SOAP is one of the most recognized formats of information organization in medicine. You can use the NCOAE SOAP Note Form to systematically move through the patient assessment while remembering and prioritizing the most essential information. For more about SOAP Notes, see our previous post, “SOAP Notes Keep Wilderness Medicine Clean.”
Sharing the Information You Gathered
Miscommunication is a frequent point of discussion during post-emergency action reviews. Here are some suggestions for ensuring that essential information is clearly communicated:
- Take a deep breath and pause before sharing important information. This technique tends to clear the mind.
- Stick to the facts (as opposed to opinion or guesses). In addition to making your information sharing clear and concise, sticking to facts helps to avoid legal or ethical problems that could arise based on an opinion, such as whether the use of substances may or may not have contributed to an accident.
- Use the phonetic alphabet when necessary to spell things out that might be misunderstood. The phonetic alphabet replaces letters with words; for example, “Alpha” in place of “A” and “Zulu” in place of “Z”.
- Consider integrating hard stops (timeouts) into your treatment policies for low-frequency, high-risk interventions to ensure that the entire team understands the situation before deciding to proceed with certain treatments.
Just the Facts
The old adage “Knowledge is power” is a poignant reminder of the important role that information plays in saving lives. However, the information we share needs to be accurate, complete, relevant, and concise. Too much information can be just as bad as too little. Stick to the facts, ask questions to clarify your own understanding, and communicate that information clearly to other members on your team. Making a conscious effort to gather and share the most accurate and relevant information possible is what gives us the power to save lives.
If you’re interested in learning more about Wilderness Medicine or our EMT Courses, click on the links.
– – – – – – –
About the Author: Todd Mullenix is the Director of Wilderness Medicine Education at The National Center for Outdoor & Adventure Education in Wilmington, North Carolina.
TALK TO US
Have any further questions about our courses, what you’ll learn, or what else to expect? Contact us, we’re here to help!
Leave a comment